
Pediatric Antihistamine Measurement Safety Check
Many dosing errors stem from confusing milliliters (mL) with teaspoons. Using a kitchen spoon can result in a 300% overdose. Use this tool to verify your measurements.
1. Medication Details
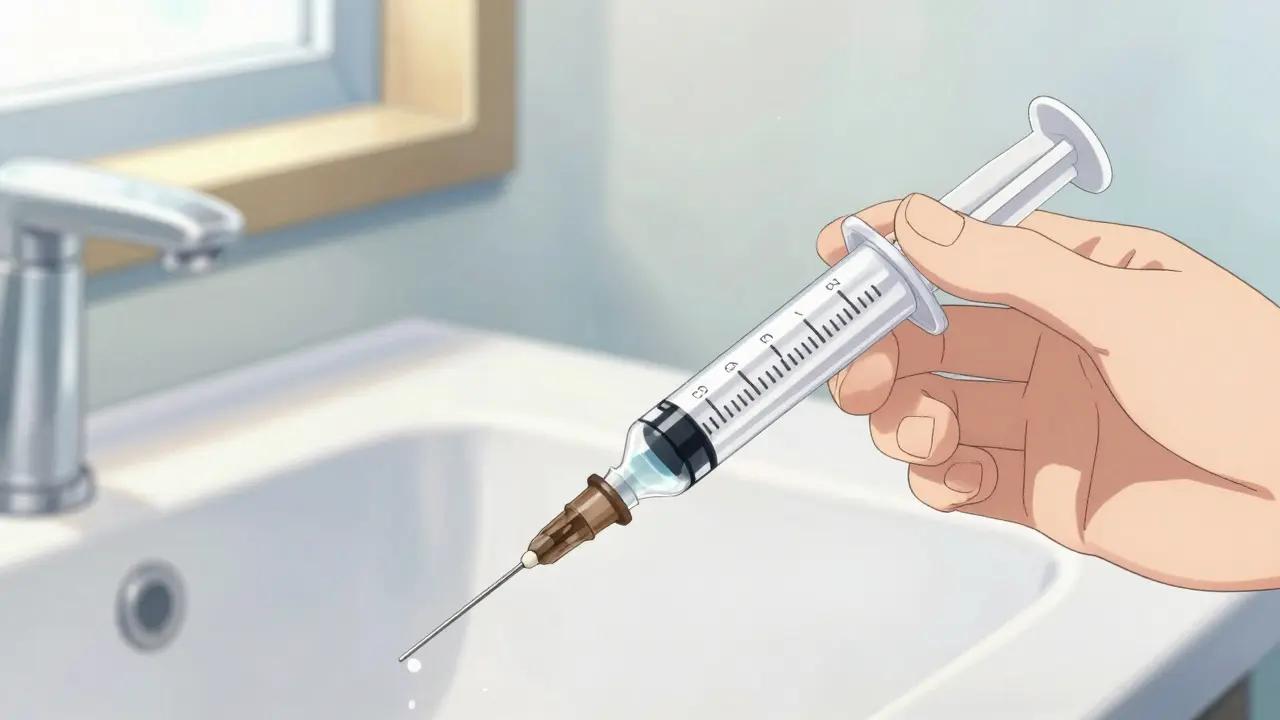
2. Safe Measurement Guide
You need exactly 0.0 mL.
(Correct Tool)
(Avoid!)
Why the difference?
Standard kitchen "teaspoons" can hold anywhere from 2.5mL to 7.5mL. Medical labels assume 5mL.
Your dose requires mL. A filled kitchen spoon could give you % too much medicine.
Medication cabinets often hide significant dangers for young children. When treating allergies, simple misunderstandings about measurement can turn routine relief into emergency room visits. According to recent data from the American Association of Poison Control Centers, antihistamines account for over 21,000 exposure cases involving children under six annually. These numbers highlight a pressing issue: proper dosing isn't just about following instructions, it is about understanding the mechanics of measurement tools and drug formulations.
We need to talk about why these errors happen. Most parents want to do the right thing, but the tools provided aren't always intuitive. Using kitchen spoons is the single biggest contributor to overdose incidents. A standard teaspoon varies wildly in volume compared to a medical measuring device. One study found kitchen teaspoons hold anywhere from 2.5mL to 7.5mL of liquid. That creates a potential error margin of 300%. If your child’s dose relies on precision, that variance is unacceptable.
Understanding Antihistamine Types and Risks
To manage safety effectively, we must distinguish between the two main categories of antihistaminesmedications that block histamine receptors to relieve allergic symptoms. They fall into first-generation and second-generation classifications, and the safety profiles differ drastically for children.
First-generation options include diphenhydramine, widely known by the brand name BenadrylDiphenhydramine. George Rieveschl synthesized this compound in 1943, and it remains the most common cause of emergency visits for antihistamine reactions today. The therapeutic index is narrow, meaning the gap between a helpful dose and a toxic dose is small. Children absorb this quickly, leading to sedation, respiratory depression, or cardiac arrhythmias much faster than adults.
In contrast, second-generation agents like Loratadinea non-sedating antihistamine approved in 1993 (Claritin) and Cetirizinea second-generation H1 receptor antagonist approved in 1995 (Zyrtec) offer wider safety margins. The therapeutic index for cetirizine is approximately 10:1, compared to diphenhydramine’s 2:1 ratio. Current guidelines from the American Academy of Pediatrics strongly advise against using first-generation options for routine management in toddlers due to these risks.
| Medication Type | Brand Name Examples | Therapeutic Index | Risk Profile |
|---|---|---|---|
| First-Generation | Benadryl (Diphenhydramine) | 2:1 | High sedation, respiratory risk |
| Second-Generation | Zyrtec, Claritin | 10:1 | Low sedation, wider safety margin |
The Mechanics of Measurement Errors
Most errors stem from a fundamental mismatch between concentration and volume. Liquid formulations vary by product and even by batch manufacturer. St. Louis Children’s Hospital dosage charts specify different volumes than Bramblebush Pediatrics for the same weight range. While minor variations exist, the real danger lies in caregiver interpretation.
Consider the scenario of diphenhydramine liquid. Standard concentration is 12.5mg per 5mL. If a parent uses a household spoon meant to hold 7.5mL, but the prescription calls for 3.75mL (¾ teaspoon equivalent), the child receives double the intended medication. This is not theoretical; the FDA Adverse Event Reporting System documented a case where a toddler received an adult dose of 50mg because the caretaker confused the concentration bottles.
The Food and Drug Administration mandates metric labeling since 2011, yet usage habits lag behind regulations. Research indicates 42% of caregivers still rely on non-standard devices. Furthermore, 34% of reported errors involve confusing milliliters (mL) with teaspoons (tsp). One milliliter equals roughly 20 drops, but relying on drop counts introduces further variability based on viscosity and dropper size.
Implementing Safe Dosing Protocols
Effective prevention starts with acquiring the right tools. An oral syringea plastic measuring device with precise markings in milliliters is the gold standard for administration. The CDC reports that using proper syringes reduces dosing errors by 62%. You can get these at any pharmacy counter free of charge when picking up liquid prescriptions. Do not accept a bottle without checking that a syringe or oral dosing cup was included.
Weight-based calculation is superior to age-based guidance. Children grow rapidly between ages 1 and 5. A blanket age recommendation often ignores weight differences that dictate metabolism rates. Always ask your pediatrician to write the dose in milligrams (mg) and milliliters (mL) on the label. Cross-referencing this with the concentration printed on the bottle ensures accuracy.
Visual confirmation helps reduce cognitive load. Studies from Harvard Medical School show that pictorial charts reduce errors by nearly half compared to text-only instructions. If you have multiple medications, keep them separated. Mixing up devices between medicines is a major cause of accidental overdoses, accounting for 44% of complaints reviewed by Consumer Reports.
- Always measure with the tip placed firmly in the child’s cheek pouch to avoid spills.
- Read the meniscus (the curved surface of the liquid) at eye level for accurate volume.
- Never give medicine by mouth before confirming the child is sitting upright.
- Store all medicines out of reach, regardless of whether they look like candy.

Recognizing Signs of Overdose
Symptoms of excessive dosing manifest differently depending on the generation of the drug. First-generation toxicity presents as extreme drowsiness, blurred vision, dry mouth, and urinary retention. Severe cases progress to seizures or difficulty breathing. Second-generation products may cause headaches, stomach pain, or palpitations rather than deep sedation.
If you suspect an overdose, do not wait for symptoms to worsen. Contact Poison Control immediately. Their hotline is staffed by pharmacists who can assess the risk based on exact weights and amounts ingested. For the United States, the number is 1-800-222-1222. They recommend calling even for suspected misuse to prevent panic-induced delays in care.
Frequently Asked Questions
Can I use a kitchen spoon to measure liquid medicine?
No, you should never use kitchen spoons. Kitchen utensils vary significantly in capacity, creating a 300% risk of measurement error. Always use the oral syringe or dosing cup provided with the medication.
Is Benadryl safe for infants under 2 years old?
The FDA and AAP strongly recommend against using diphenhydramine for children under 2. It carries higher risks of adverse effects compared to second-generation alternatives like cetirizine.
What is the difference between mg and mL?
Milligrams (mg) represent the amount of active drug, while milliliters (mL) represent the volume of liquid. You need both figures to calculate the correct dose based on the bottle’s concentration.
Why do some dosage charts give conflicting information?
Institutional guidelines can vary slightly. However, FDA-approved labels take precedence. Always prioritize the concentration on the specific bottle you purchased over general charts.
When should I call Poison Control?
Call immediately if you think a child took too much, even if they seem fine. Do not wait for symptoms to appear. Early intervention prevents serious complications.
14 Comments
March 27, 2026 Jordan Marx
The pharmacological profile of first-generation antihistamines presents distinct challenges for pediatric safety protocols. Many caregivers fail to recognize the narrow therapeutic window inherent in diphenhydramine formulations. Sedation effects can manifest rapidly due to the blood-brain barrier permeability in developing children. Respiratory depression represents the most severe consequence of accidental overdosing. Metabolic pathways process these compounds differently than adult physiology dictates. Second-generation alternatives provide a significantly broader safety margin for household administration. Cetirizine demonstrates a ten to one ratio compared to the two to one risk ratio. Measurement device variance introduces substantial uncertainty into dose calculation. Kitchen utensils lack the standardized volume required for precise medication delivery. A discrepancy of three hundred percent is observed when comparing spoons to medical syringes. Visual confirmation techniques reduce cognitive load during the administration process significantly. Weight-based calculations supersede age-based guidelines for optimal metabolic management. Institutional dosage charts may vary but FDA labels should remain the primary reference source. Proper storage prevents accidental access by curious toddlers seeking candy-like packaging. Emergency contact information should be readily available in case ingestion occurs unexpectedly.
March 27, 2026 Eva Maes
People still think using a teaspoon is fine because it worked before without immediate consequences. The statistics prove otherwise regardless of anecdotal evidence claiming safety. Dosing errors account for thousands of emergency visits every single year. Ignoring the concentration variance between brands leads to preventable toxic exposure events. Precision matters immensely when dealing with active pharmaceutical ingredients in small volumes.
March 28, 2026 Rachael Hammond
thats true though people do get scared easily i understand why. we just gotta be careful abt what we measure and make sure its right. safety first always i guess :)
March 29, 2026 Kameron Hacker
The negligence displayed in routine medication administration warrants immediate corrective action. Parents must adhere strictly to metric measurements provided by regulatory bodies. Relying on archaic kitchen tools demonstrates a disregard for established safety standards. This behavior places vulnerable children at unnecessary risk of harm. Enforcement of proper protocol is non-negotiable in pediatric care contexts.
March 31, 2026 Richard Kubíček
We should approach this situation with optimism regarding improved caregiver education. Understanding the mechanics behind the drugs empowers families to make safer choices daily. There is hope that widespread adoption of oral syringes will mitigate these preventable incidents. Community support helps reinforce correct habits rather than assigning blame alone. Knowledge is indeed power when it comes to protecting our little ones from harm.
April 2, 2026 Austin Oguche
Cultural differences in measurement interpretation contribute significantly to global health disparities. We must advocate for universal standards in liquid medication labeling practices. Metric units offer clarity that traditional household measures simply cannot provide. Standardization ensures consistency across borders and different healthcare systems globally.
April 2, 2026 walker texaxsranger
Big pharma pushes second gen drugs for higher profit margins while keeping cheap benadryl around to clear inventory. They dont want parents knowing how potent the old stuff actually is. The push for metric conversion aligns with international sales strategies not safety.
April 4, 2026 Tommy Nguyen
This is super helpful info thanks.
April 4, 2026 kendra 0712
OMG!! This is vital!! Everyone needs to read this!! Please share widely!!
April 5, 2026 gina macabuhay
It is frankly alarming how many adults continue to use improper measuring devices despite warnings. Caregivers display a shocking level of apathy towards established pediatric safety guidelines. Accidents occur because basic hygiene and diligence are neglected routinely. Negligence is not an acceptable explanation for preventable medical emergencies. Accountability must extend beyond the pharmacy counter to the home environment.
April 6, 2026 Monique Louise Hill
so scary 😱 please stay safe everyone 🙏
April 7, 2026 Sarah Klingenberg
I think it is important to remind folks to check the meniscus level properly. Reading the curve of the liquid makes a big difference in volume accuracy 😊. Keeping bottles separated avoids confusion between different meds too.
April 8, 2026 Shawn Sauve
Agreed completely on the separation part. Mixing up syringes happens more often than people admit 🙂. Just a friendly reminder to double check labels.
April 9, 2026 tyler lamarre
Common sense seems entirely absent in many modern households regarding child medication safety. Only those who read the labels properly survive these encounters without complications. Intellectual superiority determines survival rates in cases involving chemical toxicity. The majority simply refuse to adapt to basic scientific standards of measurement.
Write a comment